Ct Scan Orbital Floor Mesh

Reconstruction Of Orbital Floor For Treatment Of A Pure Blowout Fracture Sciencedirect

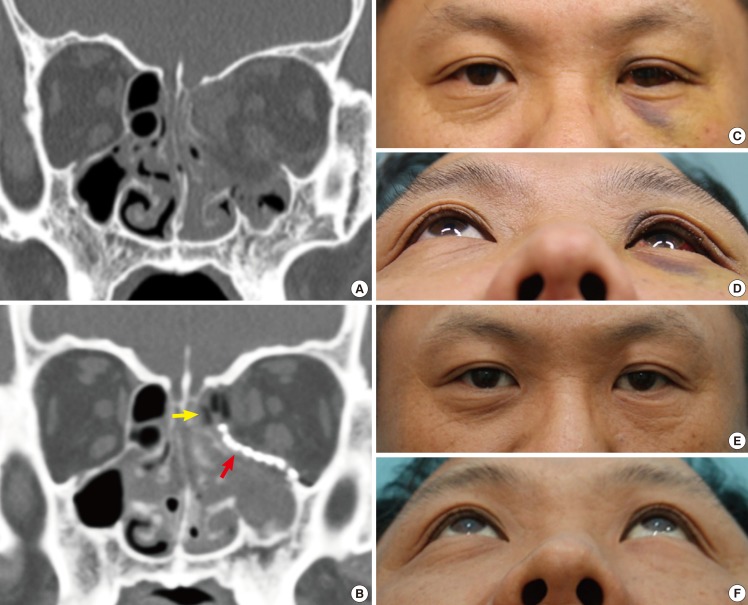
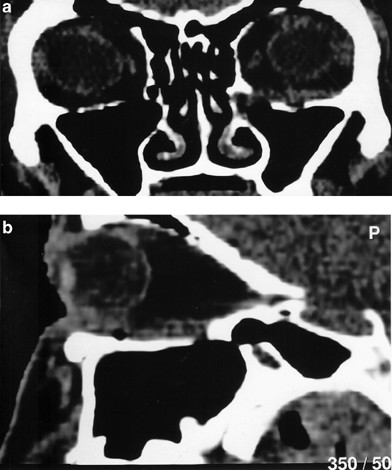
The Preoperative A And Postoperative B Ct Of The Left Orbital Floor Download Scientific Diagram

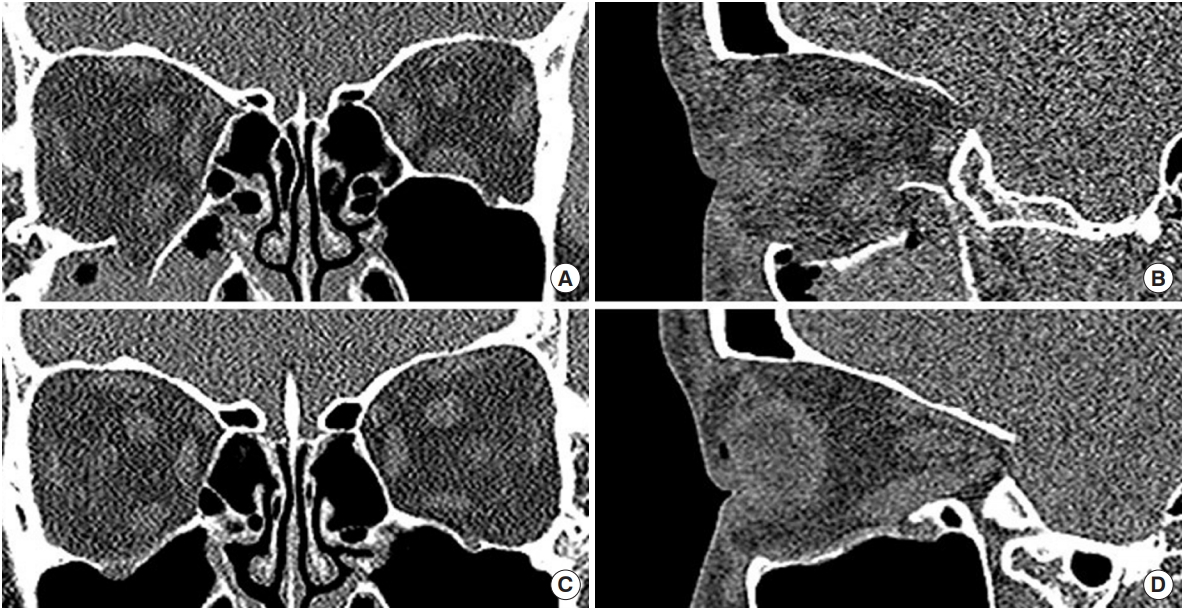
Group 1 Conv Ct Scan Images Of Patients With Unsatisfactory Orbital Download Scientific Diagram
Orbital Fractures

A Coronal Ct Scan Of The Patient Showing The Left Orbital Floor Download Scientific Diagram
Complex Orbital Fracture Repair Using Rigid Fixation Of The Internal Orbital Skeleton World Renowned Bespoke Cosmetic Plastic Surgeon Boston Dr Michael Yaremchuk
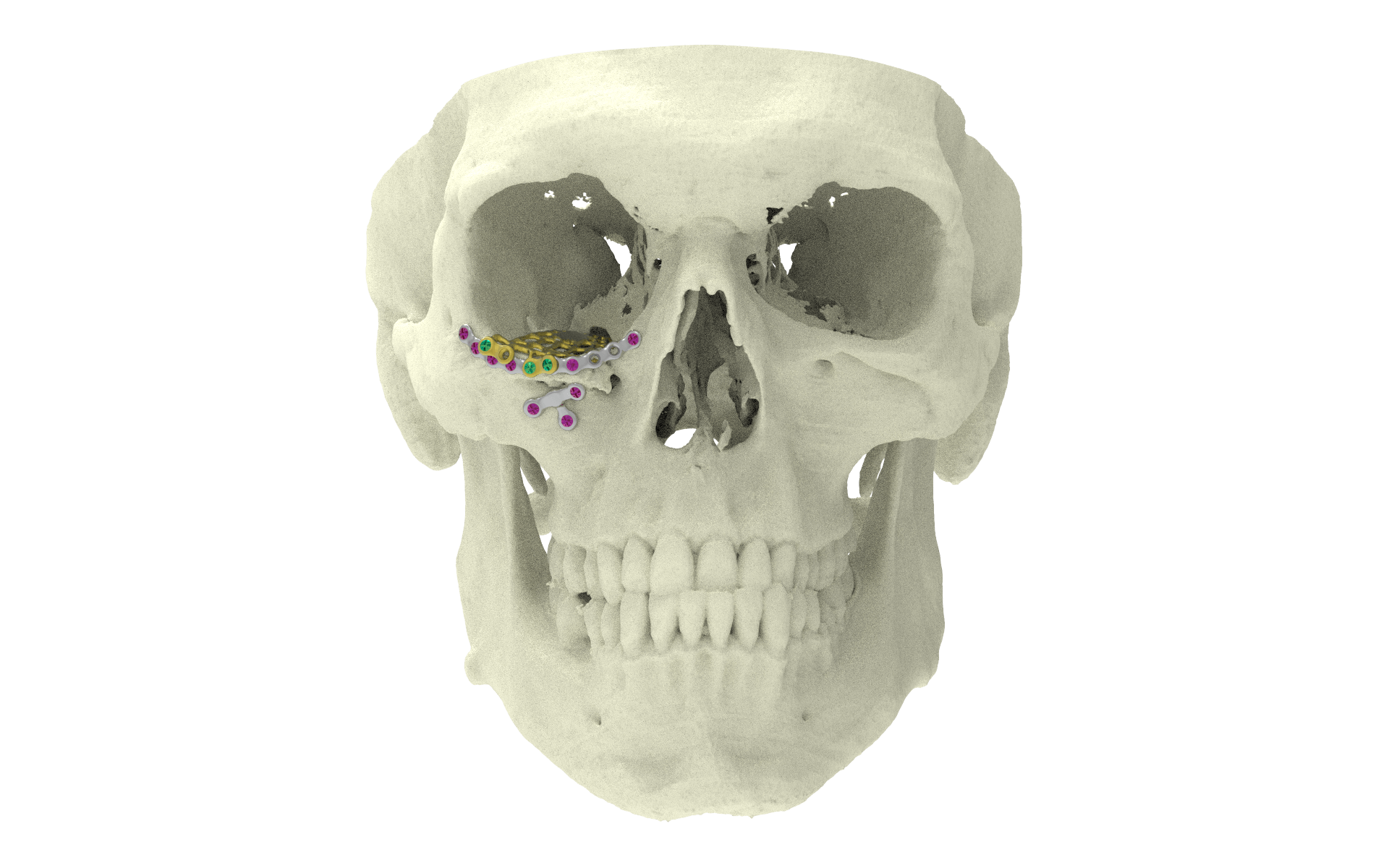
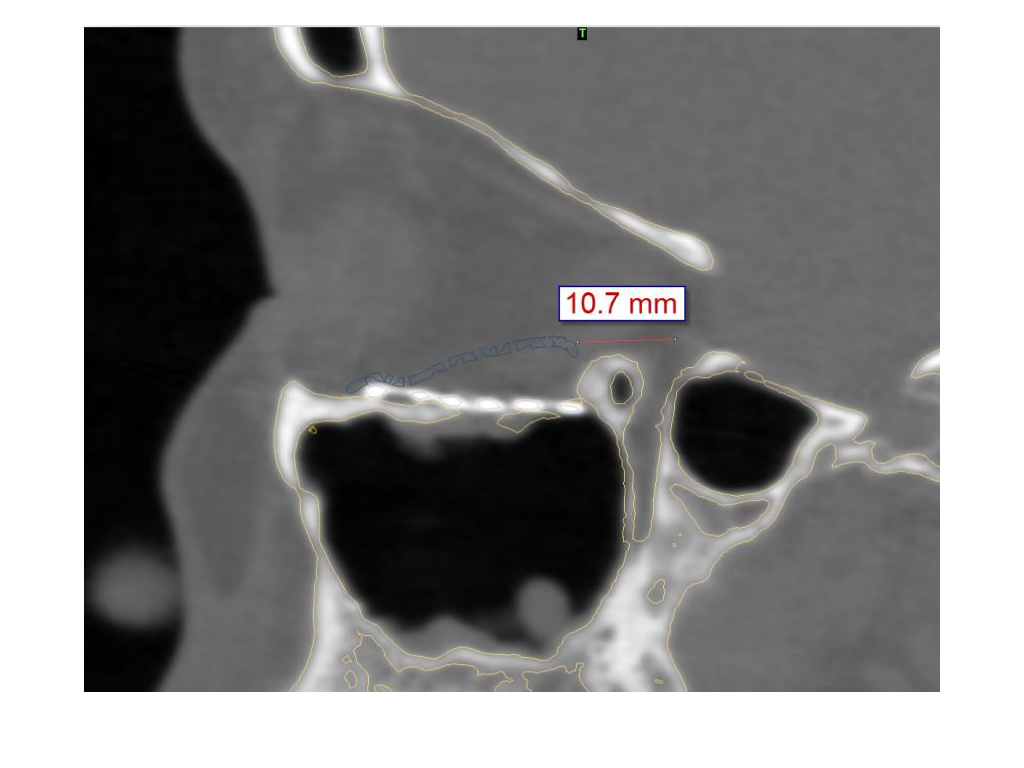
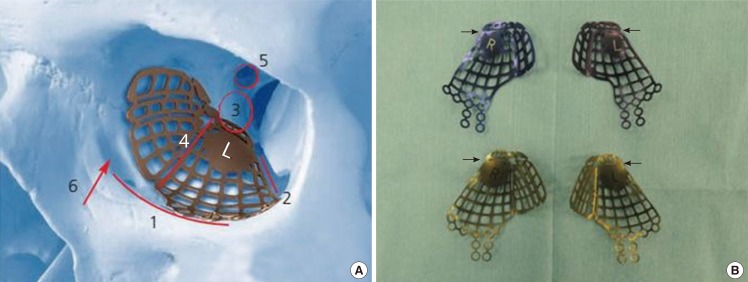
The overlying colored line in the medial wall and orbital floor area indicate the preoperative virtual planning that is superimposed on the mesh reconstructed area.
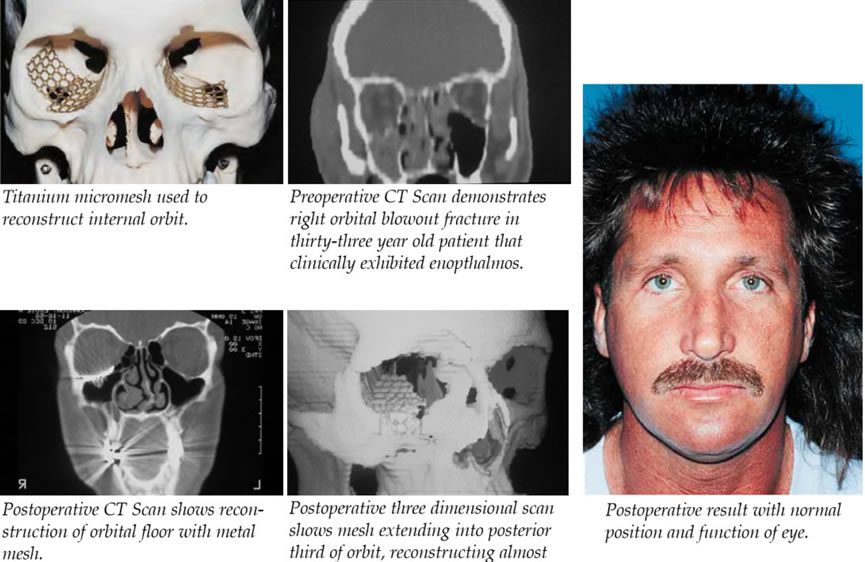
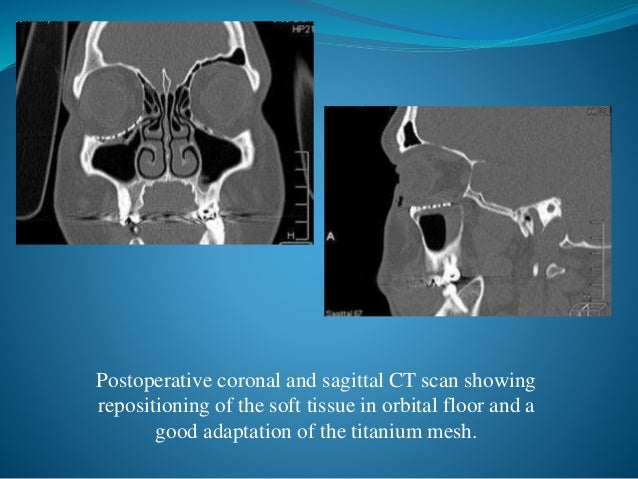
Ct scan orbital floor mesh.

Reconstruction Of Orbital Floor Using Titanium Mesh Download Scientific Diagram
Pdf Orbital Implants And Prostheses Postoperative Computed Tomographic Appearance Semantic Scholar
Orbital Reconstruction Cas Virtual Planning And Intraoperative Navigation For Orbit Orbital Floor Fracture
Materials Free Full Text Periorbital Reconstruction By Periorbital Patch Technique Using A Pericardium Based Collagen Membrane And Titanium Mesh Html
Orbital Floor Xilloc
Orbital Reconstruction Cas Intraoperative Imaging For Orbit Orbital Floor Fracture
Combined Orbital Fractures Surgical Strategy Of Sequential Repair

13 Orbital Floor Fracture Plastic Surgery Key

Type Ii Fracture A Preoperative Ct Indicated Right Orbital Floor Download Scientific Diagram
Orbital Wall Restoring Surgery With Resorbable Mesh Plate
Orbital Floor Blow Out Fractures
Epos Trade
Journal Of Otolaryngology Open Access Journals

Application Of Three Dimensional Printing Technology In Orbital Floor Fracture Reconstruction Abstract Europe Pmc

The Role Of The Dentist In Recognizing Orbital And Ocular Trauma
Biodegradable Implants For Orbital Wall Fracture Reconstruction
Http Www Ajnr Org Content 6 3 403 Full Pdf
The Silent Sinus Syndrome A Collaborative Approach Between Rhinologists And Oculoplastics Case Report And Literature Review

Nhdogou2hzgx4m
Orbital Floor Fracture An Unusual Late Complication Eye
Three Dimensional Pre Bent Titanium Implant For Concomitant Orbital Floor And Medial Wall Fractures In An East Asian Population

Pdf Management Of Orbital Fractures Challenges And Solutions

Clinical And Epidemiological Characteristics Of Orbital Floor Fractures Rebuilt With Titanium Mesh

Pdf Orbital Floor Fracture Reconstruction Using Conchal Auricular Cartilage Graft
Source : pinterest.com
